
Clinical Study at University Medical Center of Mainz (Germany)
Ulrich Betz(1), Jürgen Konradi(1), Janine Huthwelker(2), Joschua Heil(3), Friedrich Bodem(1), Helmut Diers(2), Irene Schmidtmann(4), Philipp Drees(2)
1 Institute for Physical Therapy, Prevention and Rehabilitation, University Medical Center Mainz
2 Department of Orthopedics and Trauma Surgery, University Medical Center Mainz
3 Department for Health Care & Nursing, Catholic University of Applied Sciences Mainz
4 Institute of Medical Biostatistics, Epidemiology and Informatics, University Medical Center Mainz
Introduction
Rasterstereography(1) has been proved a valid(2) and reliable(2) high precision technique to analyze the shape of surfaces(3) quantitatively based on Moiré topography. The human body surface reflects to a certain degree the spatial arrangement of immediately underlying skeletal structures. Based on back shape data and orientated on visible anatomical landmarks a suitable algorithm can be used for the estimation of the segmental spine posture. Up until now this was used for static measurements. Due to increasing computer power, it has been possible to further develop this method for the analysis of segmental spine analysis in motion. Using this our initial aim was to create standardized data regarding segmental, pelvic and shoulder rotation with respect to the corresponding gait phase for healthy subjects.
Method
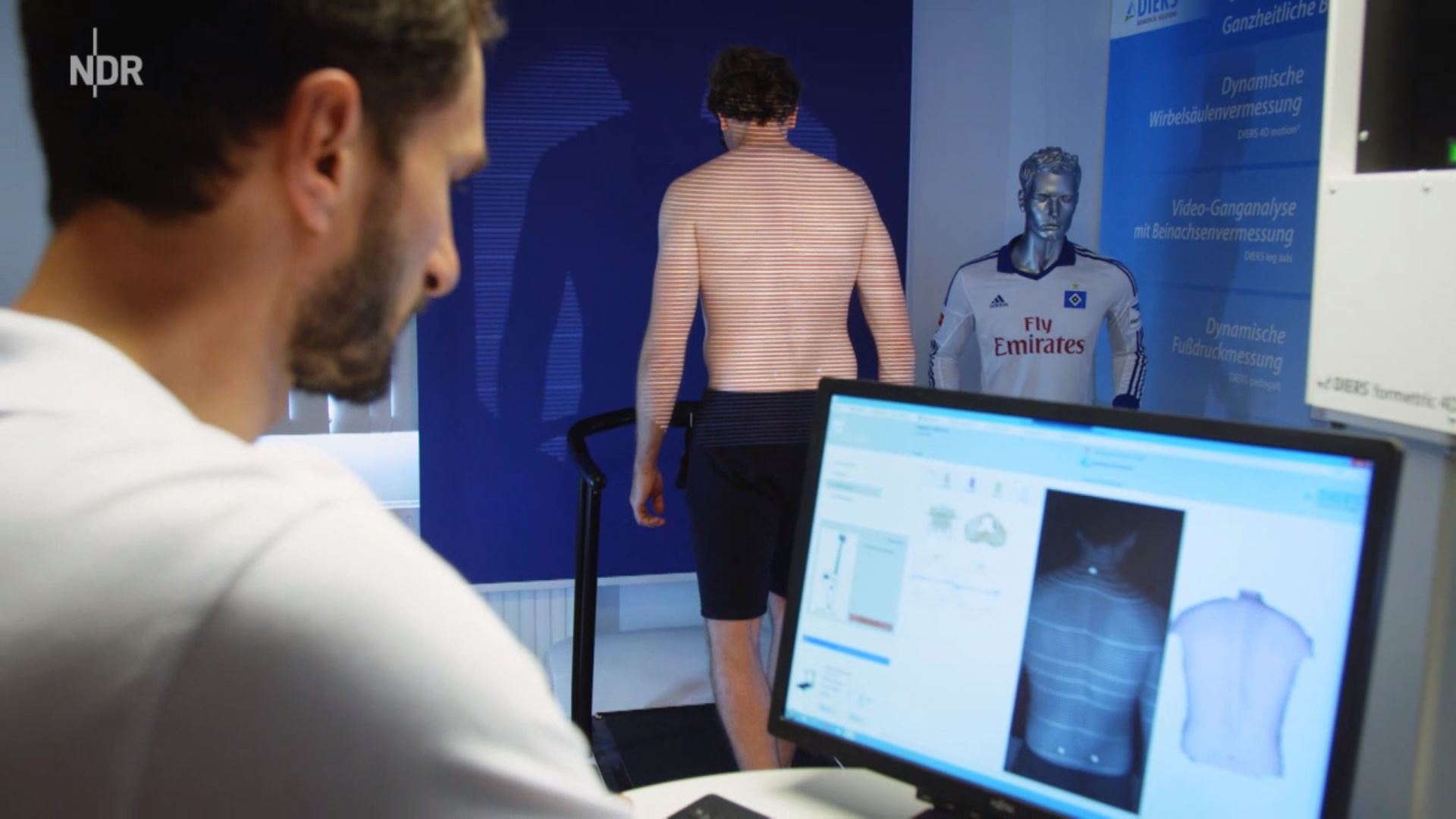
The DIERS Formetric III 4D™ analyzing system works on rasterstereography and has been used for our study. Following a strict study protocol we have examined a total of 134 pain free and healthy male and female subjects with an age range from 18 to 70 years. Three complete gait cycles per participant walking on a treadmill at a speed of 2, 3, 4, and 5 km/h were analyzed with 60 pictures per second. For every single frame the spinal segment-related geometry in three dimensions was calculated based on more than 400.000 spatial coordinates referring to the backside trunk shape. Hence, we possess 3-dimensional spatial data for each segment.

Results
To recognize and understand the system within the existing variety we extracted a subset from the full amount of data. Therefore, in our presentation we concentrate on rotation data for the pelvis, L4, T12, T8, T4 and the shoulder girdle. Graphs chosen should give an impression of the versatility of the rotation patterns.
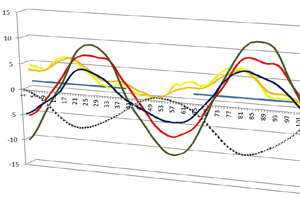
1. Mostly in line with our expectations we found strongly periodic, sinusoidal oscillations revealing a phase shift between the pelvis and the upper thoracic segments with it’s maxima facing each other: At the beginning of the right foot’s stance phase the pelvis is maximally rotated to the left, reaching the zero point in the middle of the stance phase. L4 constantly follows the rotation of the pelvis. T12 tends towards the zero point and is still in the alignment of the pelvis. Maximum antagonistic rotation is mostly displayed by T8. T4 is also rotating in the opposite direction of the pelvis but to a lesser extent. The amplitude and the period are intra-individually constant. Maxima and minima of the pelvis and the thoracic segments face each other, meaning an equalisation of the pelvic rotation by the thoracic spine. The shoulder shows little movement.
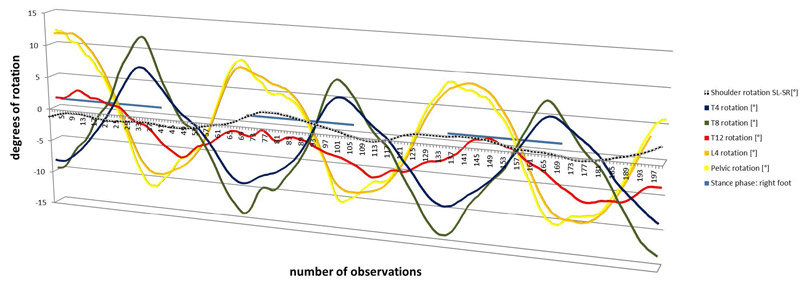
Figures: Positive values show rotation to the left and vice versa. Abscissa reveals the number of observations, always starting with initial contact of the right foot. Duration of the stance phase is marked with a horizontal blue line.
2a. Nonetheless, there is a broad variation within specific manifestations for each individual:
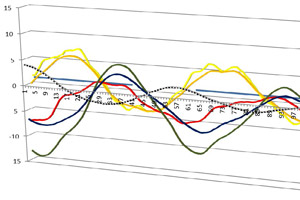
Rdxy 9001 | 5 km/h:
Pelvis starts at the zero point; reduced phase shift between pelvis and thoracic segments, pelvis initiates rotation and thoracic spine follows
Rdxy 9013 | 5 km/h:
Rarely seen reverse pattern, pelvis and all segments rotating in phase indicating walking in amble
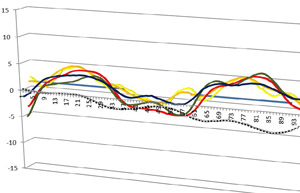
Rdxy 9038 | 5 km/h:
Still sinusoidal but with triplets of swings of the pelvis and the segments
Rdxy 9027 | 5 km/h:
Late maximum of the pelvis, reduced thoracic segments phase shift, shoulder shows antagonistic oscillation to the pelvis
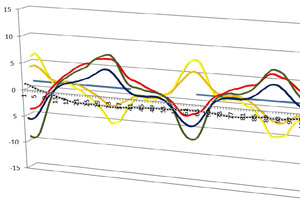
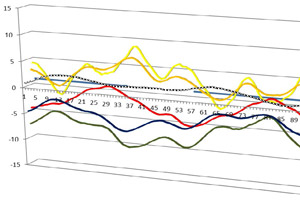
Rdxy 9023 | 5 km/h:
Pelvis starts nearly at its maximum directly facing the thoracic segments, rotation towards the maxima becomes very steep
2b. Additionally, we see variation due to the alignment during stance. Rotation patterns can be shifted towards the left or the right side. After substraction of the rotation value for stance a correction occurs levelling the rotation around the zero point.
Changes in rotation patterns before (a) and after (b) correction: Initial pattern is shifted to the right as a whole, after substraction of stance rotation a correction occurs levelling the rotation around the zero point


Discussion and Conclusions
As demonstrated we observed a broad pattern of inter-individual variation. Therefore, averaging the results and creating a standardized ‘normal’ rotation pattern does not seem to be the right step at the moment, since comparison of the physiological highly individual profiles with a confidence interval around an median easily bears the risk of pathologizing it. Thus, we had to revise our initial aim. Maybe not comparison of similarity but rather of differences, for instance the difference of the phase shift, e.g. between the maximum rotation of the pelvis and the reverse rotation of T8, can yield characteristic types of movement. Also deriving broader more basal criteria for standardization might be a future goal. To ensure validity of our measurements we want to apply repeated measurements within the same individual, to see whether the intra-individual pattern remains, revealing an personal ‘footprint’. A further objective might also be the inclusion of pathologies for comparison of physiological and pathological variations.
References:
(1) DRERUP, B. & HIERHOLZER, E. 1994. Back shape measurement using video rasterstereography and three-dimensional reconstruction of spinal shape. Clinical Biomechanics, 9, 28-36
(2) BETSCH, M., WILD, M., JUNGBLUTH, P., HAKIMI, M., WINDOLF, J., HAEX, B., HORSTMANN, T. & RAPP, W. 2011. Reliability and validity of 4D rasterstereography under dynamic conditions. Comput Biol Med, 41, 308-12.
(3)KNOTT, P., STURM, P., LONNER, B., CAHILL, P., BETSCH, M., MCCARTHY, R., KELLY, M., LENKE, L. & BETZ, R. 2016. Multicenter Comparison of 3D Spinal Measurements Using Surface Topography With Those From Conventional Radiography. Spine Deformity 4, 98-103.





{kind=link}
{kind=link}
{kind=link}